Previous blog ´War against a virus´ was on the general features of the virus. Here I try to feed the information regarding the virus (SARS CoV-2) and the disease it causes (COVID-19), which may help you to understand better this hidden enemy. Science is on the learning curve for this novel virus. For that reason, journals, databases, media are flooding with new information regarding this disease (take them with a grain of salt, since most of them are non-peer reviewed; that means not well scrutinised by experts in the field). Please check the ´references´ section for original papers. Note, as we learn more about this virus, we have to update, change our thoughts and strategies to fight against this disease.
The top on the list is ´Hydroxychloroquine´ treatment
Though US President and other political leaders are pushing on this anti-malarial drug hydroxychloroquine-HCQ (´´a gift from heaven´´ according to Mr. Trump) for COVID-19, the Scientific community is cautiously waiting for the scientific evidences from clinical trials. The demand for this ´game-changer´ drug is so high that US President Trump was literally threatening India, the biggest manufacturer of HCQ, for lifting its export-ban.
Some hospitals in Sweden and France stopped using HCQ for COVID-19, due to severe cardiac and vision side effects. Further, the controversial original scientific article (that claimed the antiviral activity of HCQ for SARS CoV-2) is facing fierce criticisms from scientific community and investigation from the journal/publisher. Researchers are coming with conflicting results on this ´Corona drug´, the main drawback in common about these studies is very low sample numbers hence are considered as pilot studies. This drug is effective in some chronic disease conditions (like arthritis, lupus). Due to overhyped anecdotal evidences as anti-COVID-19 drug, people all over the world are stockpiling this drug, posing a huge problem for those patients relying on this drug for their chronic clinical conditions. Please wait some more weeks/months for the verdict from WHO´s solidarity megatrial, to understand whether HCQ will be a safe ´silver-bullet´ or is just a ´false hope´?
Remdesivir- the magic bullet?
Ebola virus is also an RNA virus and uses a similar mechanism to replicate inside the infected cell, remdesivir will act on the copier machine of virus-RNA dependent RNA polymerase (the key protein for the viral replication) and inhibit it. Remdesivir was designed for Ebola treatment. There are promising preliminary data that this drug might work effectively to inhibit RNA polymerase of SARS CoV-2 too. Recently, a study published in a scientific journal (NEJM) showed promising results from this drug. This study was carried on a small group of nearly 50 patients. Intriguingly, the outcome was judged based on improvement of clinical symptoms while no analyses were on viral load! Any concrete conclusion from this study is difficult to make. A randomized control study is warranted and hence here also we need to wait for the judgment from WHO´s megatrial, on remdesivir.
Ivermectin- from anti-parasitic drug to antiviral drug?
Interestingly, a known FDA-approved anti-parasitic drug Ivermectin showed antiviral activities on SARS CoV-2. This drug previously showed some effects for other viral diseases had antiviral effects in SARS CoV-2 (mechanism is unknown), but in cells in a dish, that too at a higher concentration than recommended. Extending these results from the cell-culture to humans is not very easy though. Need a long way to go!
Desperate attempts- trying everything in the pharmacy shelf
Japan is trying themselves and donating Favipiravir to other countries (an effective influenza drug). Mechanism of action is by inhibiting the copier machine of a virus (a common mode of action of many antivirals). Trials are currently going on to get approval for this drug for treating COVID-19. In Denmark, a trial is going on another drug called Camostat mesylate– that acts on the cellular protease TMPRSS2 (remember the diagram from previous blog- a protein that helps the virus to get inside the host cell). Note, here the strategy is different the drug targets a cell protein hijacked by the virus to do its job.
A simple mask to prevent the spread.
Recent studies suggest that SARS CoV-2 may be viable in the droplets an infected person sheds while he talks, sneezes or coughs. These droplets can travel a short distance before it falls down on the surfaces. Once outside the host, viability of the viruses depends on environmental conditions. Under laboratory conditions this virus can stay stable for upto 3 days on plastic surfaces, upto 2 days on steel and a day on cardboard surfaces. Interestingly, SARS CoV-2 was viable upto 3 hrs in aerosols (but infectivity depends on the inoculum shed). Prof. George Gao, a top virologist and director-general of Chinese Center for Disease Control and Prevention (CDC version in China), expressed his concern that it is a ´big mistake´ not wearing masks indicating micro-droplet mediated transmission should not be ignored. The evidences forced many countries to change their mind and recommended the usage of mask while going out. Assuming that asymptomatic spreaders are in significant numbers and since they have similar viral load as symptomatic patients, it is wiser to use some kind of covering to your face. One concern was this will take away the masks for health workers, but experts from CDC now recommend the usage of atleast a home-made mask while going out.
Serological test- antibodies
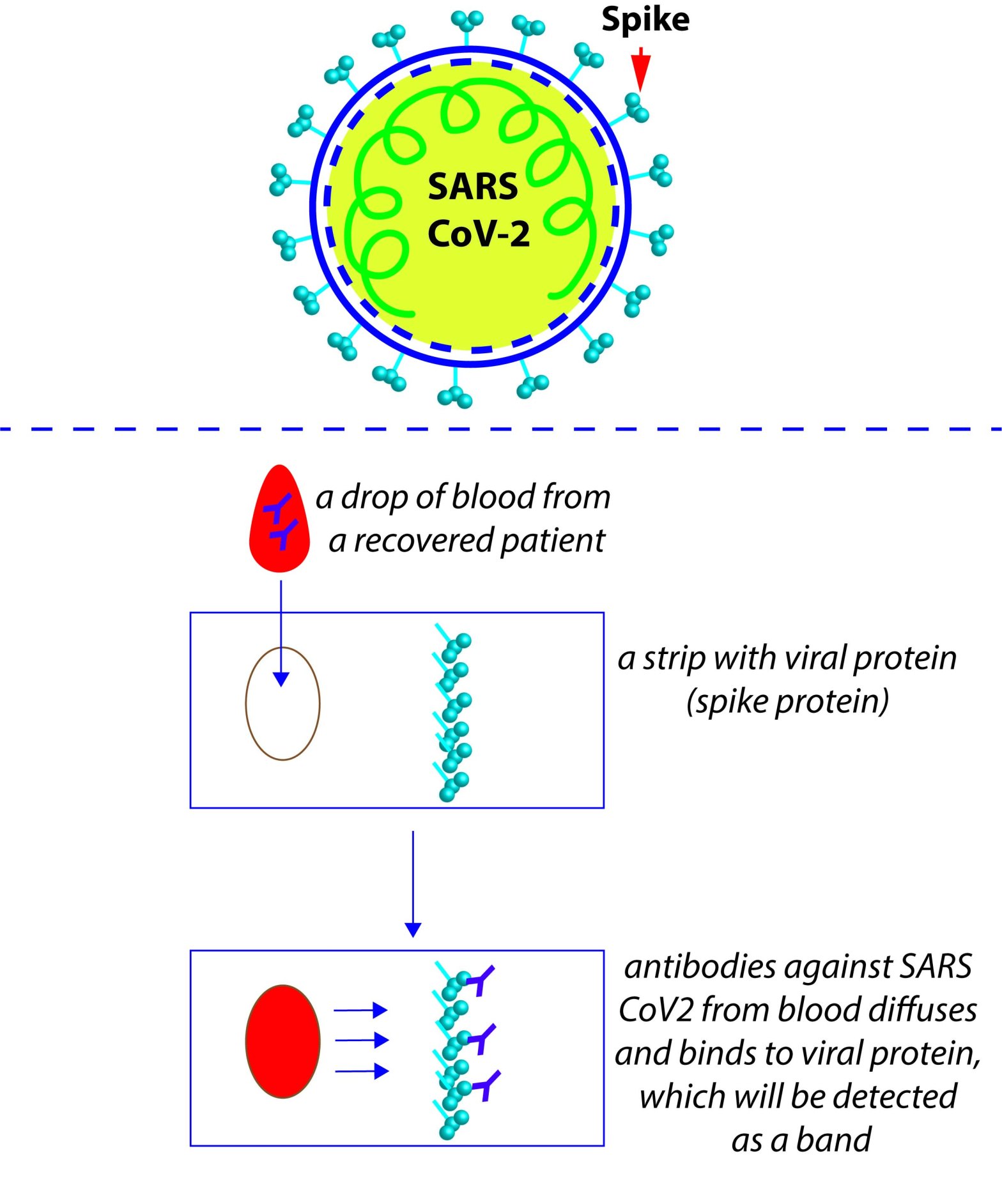
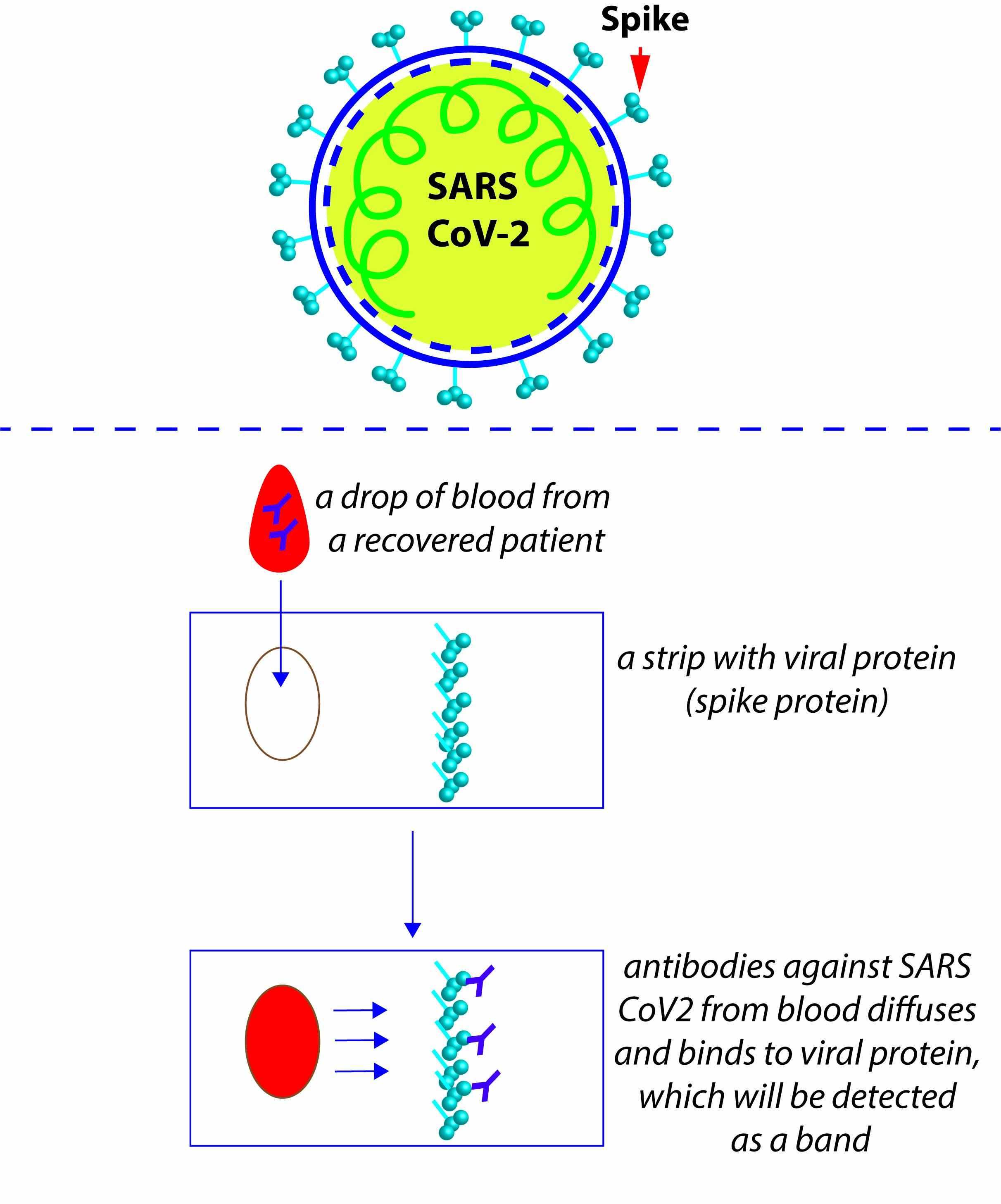
RT-PCR based testing can detect the ongoing infection but cannot detect the survivors who were asymptomatic or had mild symptoms. This is because RT-PCR detects the genetic material of the virus, once our body recovers from the viral infection its genetic material will not be present. On recovery, even though no SARS CoV-2 viruses are present in the body, our body gains antibodies for a longer time against this virus (assumption based on similar Corona viruses). Antibodies/immunity created against this virus by our body act as warriors against the same virus in case of second attack. There is another way that we can detect the survivors- using an antibody-based serological test. A drop of blood from your fingertip on a testing strip will tell whether you already had a silent infection and if you are immune to SARS CoV-2 virus. The strip holds pieces of viral protein (usually the viral spike protein), which will recognise and bind by the anti-SARS CoV-2 antibodies present in the survivor’s blood. This specific binding between the viral protein and the antibody can be detected as colored bands by the reaction chemistry, on the strip (like the pregnancy detection strip). With such a simple test one can roughly detect whether you had a recent infection or an ongoing silent detection. An oversimplified version of the serological test for COVID-19 is shown below (to understand the logic behind the test).
If we assume that the immunity gained by COVID-19 survivors sustain for couple of seasons (we are learning about it), then with precise immunological tests we can determine the residents who are immune to a subsequent infection. Such a SARS CoV-2-immune population can get back to work, volunteer helping the vulnerable and bring the economy back on track. One major issue that we are facing with regard to this test is the sensitivity and accuracy (note, the sensitivity of RT-PCR is high in detecting an ongoing infection). Many vendors are in the market with such COVID-19 kits, whether all of them meet the quality criteria is a big question.
Bouncing back of SARS CoV-2; a second wave?
Now many countries have flattened the curve, and it’s time to get back on our duties. Even if many of us escape from this ´first wave of SARS CoV-2´, this bug is going to be around for several months. Since complete isolation for a longer period is literally impossible, we may expect bouncing back of virus mostly by importing virus from other countries with ongoing cases. Wuhan, the epicenter of this outbreak is open now. China harnessed this highly transmitting disease by Draconian measures of strict lockdown and social distancing measures. This means the population might have failed to attain the herd immunity, hence there is greater chance of second wave of COVID-19 in China in coming days.
Antibody levels are not same in survivors: A recent non-peer reviewed study analyzed that neutralizing antibody levels (antibody that binds the virus and thereby inhibiting the virus from entry and replication) from several recovered patients (they had only mild symptoms!). They observed difference in the level of neutralizing antibodies in young, middle-aged and elderly (surprisingly, young recovered showed lesser antibody levels than others). This study got attention, based on this study many warned that if real, this will lead to second infection in the recovered patients (rebound). Moreover, this study warrants careful titration of serum from recovered patients, for convalescence therapy. The caveats of this preliminary non-peer reviewed study are many folds. The antibody they analyzed was only one kind-a neutralizing antibody against spike protein, while our body makes antibodies against several other viral proteins. Further, our body has other mechanisms to fight against a virus other than with neutralizing antibodies. Most important is they don´t know the initial viral load of these patients- which will have an impact on their antibody levels.
Sweden-the black sheep in the flock
While almost all the countries were following a similar approach of strict social distancing measures and lockdown to tackle COVID-19, Sweden to a great extend is not following the WHO guidelines in this COVID-19 fight. Though not very explicit, they are looking towards the herd immunity- an unknown approach for a novel virus. Already they are facing fierce criticisms on this matter not only from the scientific community but also from leaders outside. It may be too early to say whether their approach is a blunder, but the preliminary data is not very promising to their bold approach (comparison to their Scandinavian neighbors).
BCG vaccination for tuberculosis and COVID-19- two birds with one stone?
Again, another non-peer reviewed manuscript came up with the correlation of BCG vaccination (protector of tuberculosis) and less prevalence of COVID-19 in countries with BCG still in their vaccination policy. BCG vaccination given at birth, in many countries may not provide life-long immunity though. The argument is that these vaccinations may boost up the immunity (trained immunity) in the vaccinated which will augment our body´s fight against COVID-19. While WHO does not recommend BCG vaccination for prevention of COVID-19, they are waiting for the outcome of clinical trials (BCG vaccination to healthcare workers treating COVID-19 patients). More data, as well as a molecular mechanism is needed for supporting this correlative observation. Quite ambitious to expect a specific vaccine to fight against multiple diseases by boosting the immune system (mechanism not well understood), but why not?
Strains-will that matter?
A recent article from Cambridge University researchers reported 3 types of the deadly coronavirus are spreading around the world. They analysed the genetic sequences of SARS CoV-2 virus isolated from the patients from different parts of the world and found three distinct variants- A, B, and C. A-type is the ancestral one but interestingly not the most common one in China. As you understood from my previous blog, this RNA-virus undergoes mutations (though to a lesser extent than flu virus). These mutations get accumulated on transmissions and forms different genetic types or strains (this does not necessarily mean that there will be a huge shift in its pathogenic features). Analysing these variations help researchers to keep track of the propagation of SARS CoV-2 from one place to another.
Seasonal pattern of Coronaviruses
Researchers from University college of London studied the seasonality preferences of three other coronaviruses (same family as SARS CoV-2) and came up with the conclusion that these viruses show a preference towards winter. The study is under peer review, and is not specifically on SARS CoV-2 (on CoVs in general), but it gives hope to many countries that are suffocating with COVID-19, where the winter is almost ending. If true, this is good news to Northern hemisphere while it gives alarm bell to the South, for preparedness.
Pandemic endgame
If this virus lingers around several months in different regions, it may not be easy to extinguish this fire completely. Countries who successfully contained this virus now, but not attained herd immunity will have to tighten their borders to prevent influx of cases from abroad. Sporadic outbreaks will force countries to reinstall the lockdown measures in those regions. If the social distancing works in mitigating the rapid virus spread and deaths, we may need to extend it for longer time periods to take care of the vulnerable. In the absence of a quick silver bullet (safe drug or vaccine) a significant population will be infected, and the survivors may establish herd immunity. Eventually, the virus cannot encounter viable hosts and subsides, but this natural approach is at the cost of millions of deaths! Coronaviruses generally show seasonality, it may subside during summer in many countries (but it is hard to speculate on any novel virus). Conversely, places where the environmental factors become favorable for viral propagation in coming months should prepare proactively on personal protective equipments, medicines, ventilators etc. Assuming that the immunity attained by patients recovered from COVID-19 will sustain for couple of seasons, then with the help of precise immunological tests we can determine the residents who already got and are immune to COVID-19. Those who are immune can safely get back to work.
One thing is for sure, this tiny string of RNA exposed the incapability of the health systems of even many developed countries in managing a pandemic. We must learn from this episode and prepare for such pandemics which may happen in future.
Video of this blog
Physics of the sneeze
https://www.youtube.com/watch?v=bFxgVkslD-k
References:
Original article on HCQ and its antiviral activity
https://www.sciencedirect.com/science/article/pii/S0924857920300996?via%3Dihub
Concerns by the journal on the HCQ study
https://www.isac.world/news-and-publications/official-isac-statement
No evidence HCQ antiviral activity
https://www.ncbi.nlm.nih.gov/pubmed/32240719
Trump Threatens India
https://www.bbc.com/news/world-asia-india-52180660
Solidarity Megatrial
Masks are important
https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/diy-cloth-face-coverings.html
Asymptomatic patients have similar viral load
https://www.nejm.org/doi/full/10.1056/NEJMc2001737
Remdesivir
https://www.nejm.org/doi/full/10.1056/NEJMoa2007016
Ivermectin
https://www.sciencedirect.com/science/article/pii/S0166354220302011
Camostat mesylate
Neutralizing antibody responses in recovered patients
https://www.medrxiv.org/content/10.1101/2020.03.30.20047365v1
Silent carriers
https://science.sciencemag.org/content/early/2020/03/24/science.abb3221
Serological tests
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)30788-1/fulltext
Second wave
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)30845-X/fulltext
BCG vaccination and WHO
https://www.medrxiv.org/content/10.1101/2020.03.24.20042937v1
3 variants of SARS CoV-2
https://www.pnas.org/content/early/2020/04/07/2004999117
Seasonality of CoVs

Well written summary of the latest updates. I’m also in agreement to the endline of this article that there doesn’t seem to be an end to this pandemic in the near future.
LikeLike
Thanks Priya 🙂
LikeLike
Excellent , simple and fully scientific analysis of the present situation. Good job chetta , thank you
LikeLike
Thanks Shantha 🙂
LikeLike
well written .may be guidelines for scientists who are researching on their vaccine.
It is no so easy language layman can understand.
LikeLike
Thanks 🙂
LikeLike
You have done a beautiful hardwork and research. This will definitely be a valuable information for those who are working and researching in this field.
LikeLike
Thanks, I was just communicating Science 🙂
LikeLike