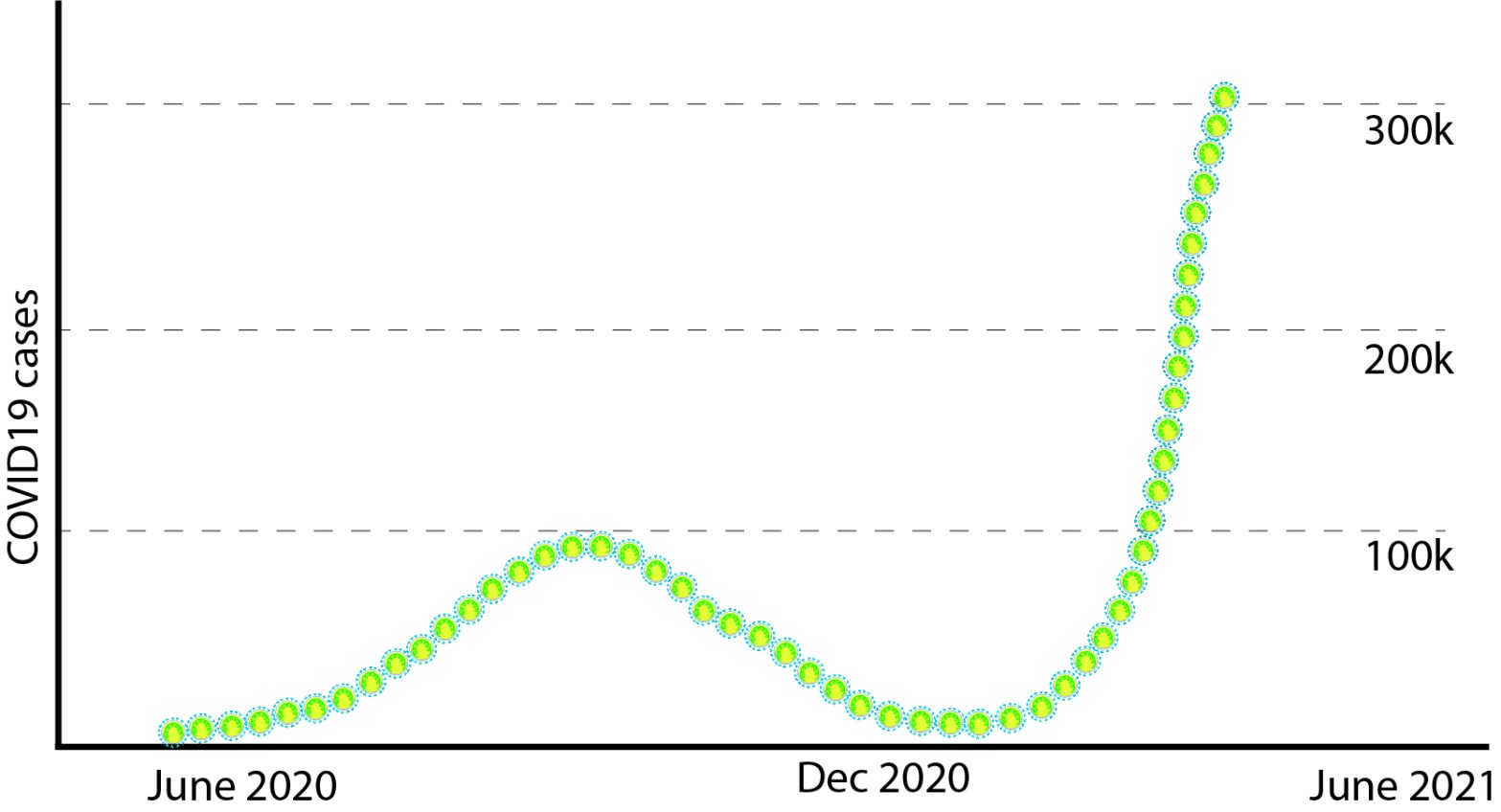
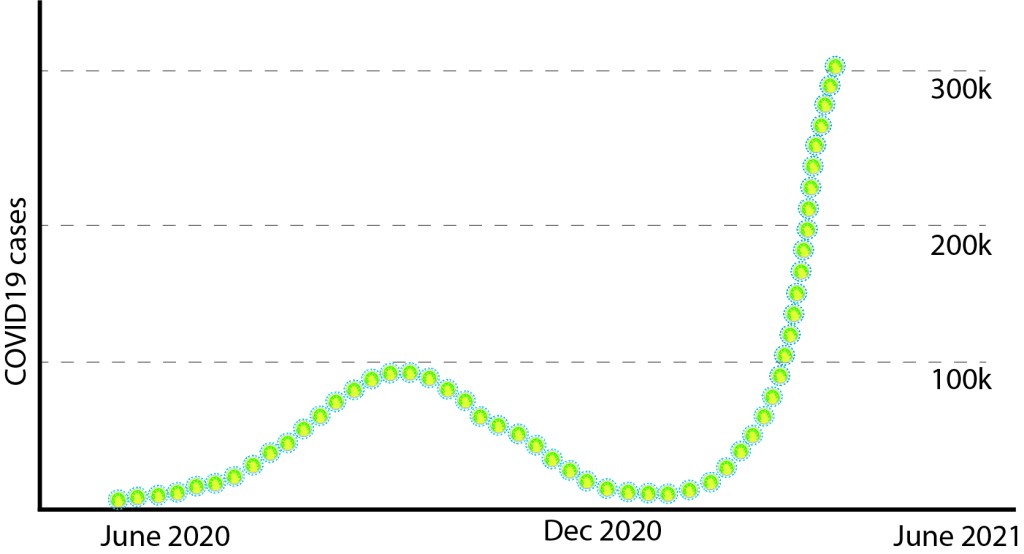
From a premature victory declaration over COVID-19, now India is under the ruthless grip of the enemy in new disguise. After curtailing to less than 10,000 daily cases towards the end of the first wave, now a staggering over 350,000 daily cases and nearly 3200 daily deaths! Neglect on mitigation measures, worse policies and inadequate preparations, false belief that India had beaten COVID-19, vaccine hesitancy, recommendations of pseudoscience, opening of theaters, no restrictions on mass religious gatherings, elections in several states, mammoth political rallies and protests, emergence of variants, all these factors played their role to induce this massive tsunami of Coronavirus, with record daily cases, overwhelming hospitals and crematoriums! India was in an advantageous position to plan in advance, we were seeing the merciless massive second wave sweeping through several western countries and instead of preparing for the inevitable second wave, we neglected the signs and assumed that pandemic is over for us. The comparatively less damage inflicted by first wave (against the predictions), also gave the false impression that we are done with the pandemic, but this virus was not done with us, yet. Propelled by early victory declaration, masses laxed strict mitigation measures which furnished a cozy incubator for emerging variants (viruses are obligatory parasites- they need a host to propagate, the reason why social distancing and mitigation measures are relevant) and an easy take off- now a tsunami is in front of us! Postmortem analysis on factors that fire-triggered this wave is crucial to avoid future mistakes, but amid this disastrous wave let´s focus on solutions to bring this big wave down, study the variant(s) under investigation and escalate the vaccination program.
B.1.617 aka wrongly named ´double mutant´
Variants or mutants always emerge, nothing surprising about it. Mutations are changes in genetic material (DNA or RNA) that may cause changes in the proteins. The process is not something special to SARS CoV2 virus, such coping errors happen when genetic materials (DNA or RNA) are copied. Some of the variants attain favourable features to propagate and flourish (survival and propagation of the fittest). To confirm that they are variants, genomic sequencing should be done in large scale, i.e., a high number of viral genome sequencing from the infected is the way to detect variants and take subsequent timely actions to contain it. The current massive surge in India could be due to a dominant variant or multiple variants or could be due to factors mentioned above like relaxation in mitigation measures. The variants B.1.1.7 (first reported from UK), B.1.351 (first reported from SA) and B.1.617 (first reported from India) are in direct competition in many places in India, and the one with evolutionary advantages will take over the other and could become the dominant (like the variants competed out the original virus first reported from Wuhan, China). B.1.617 is currently more prevalent in the genome sequenced samples and uploaded in global database Global Initiative for Sharing Avian Influenza Data (GISAID) recent weeks. Even though anecdotal reports on changes in clinical behaviours of the disease are appearing, thorough investigations are needed to make any conclusions.
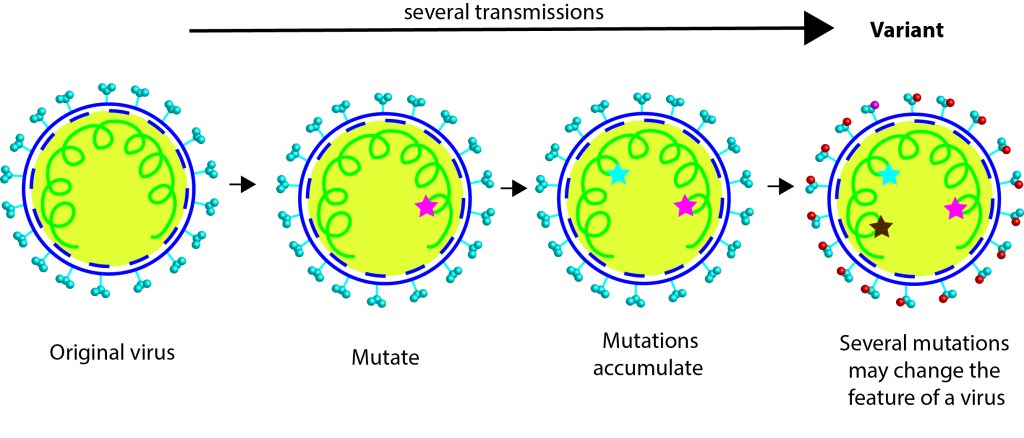
The popular media named the variant B.1.617 as ´double mutant´ (as an easier alternative to the confusing strings of letters, numbers, and dots) since it bears two key mutations reported in two other notorious variants. L452R mutation-present in the dominant strain first detected in California, and E484Q mutation- like the one present in the variants first reported from South Africa and Brazil. Furthermore, the variant B.1.617 has 13 mutations in total (not just 2) compared to the original COVID19 strain first reported from Wuhan, China. For those who are interested in detail, B.1.617 accumulated more than 2 mutations, namely D111D, G142D, L452R, E484Q, D614G and P681R, even in the spike protein including within the receptor binding domain (RBD). The RBD mutations L452R and E484Q along with P681R in the furin cleavage site, may result in better transmissibility of this variant. The two RBD mutations may result in decreased binding to selected monoclonal antibodies and may affect their neutralization potential. Thorough investigations are warranted to determine the transmissibility, infectivity, and virulence of this variant under investigation B.1.617 and the effectiveness of the current vaccines against it.
Earlier, it was reported that nearly 50% of the inhabitants in Delhi were seropositive, which means nearly half of the inhabitants had antibodies against the Corona virus due to symptomatic/asymptomatic infections. The resurgence of the second wave could be driven by waning immunity in those infected or evasion of immunity by the new strains or both, which is worrisome. That is, over time, as the immunity attained by first infection got waned, meanwhile more contagious variants popped up and ignited a surge that turned into a tsunami. Caution: If B.1.617 does increase the chance of reinfection or breakthrough infections in the vaccinated, and manage to cross borders; then probabilities are high B.1.617 could drive resurgence of COVID-19 in other parts of the world where a population’s immunity (obtained from natural infection or vaccine) is on the decline. Several countries learned from their experiences from devastating 1st and 2nd waves, and are now proactive by canceling flights from India. In a closely connected world, by the time we learn more about a variant of concern, it might have propagated across many borders- the B.1.617 is already in circulation in several countries- the horse is already out of the barn!
B.1.617 genome was detected back in 5 Oct 2020, appeared in the global database Global Initiative for Sharing Avian Influenza Data (GISAID) but during that time the first wave was in an indisputable descending trend, remarkable vaccine trial results were coming out, hence whether we gave sufficient attention to gear up our genomic surveillance and analyze the characteristics of this variant (infectivity, transmissibility etc.) is doubtful. Important to note that original SARS CoV2 virus was quite successful in propagation compared to any other viruses and managed to spread waves around the globe in a short time. A variant with ´more transmissibility´ is in a way more detrimental in choking the health system than one that causes ´more severe disease´. Suppose if B.1.617 is more transmissible or virulent, what could we do differently to treat this disease is a question? Whatever mitigation measures currently we follow, that includes social distancing, masks, hand hygiene, avoiding indoor gatherings etc. should be continued for longer time, in fact more strictly, until a significant percentage of population gets vaccinated.
Very recently, a promising non-peer reviewed report came out suggesting that the sera from the natural COVID-19 infected and recipients of BBV152 (Covaxin) were able to neutralize B.1.617, emphasizing the seriousness in boosting the COVID-19 vaccination program in India. Though neutralizing efficiency of sera from other COVID-19 vaccines against B.1.617 weren’t reported, they should also protect us from critical illness during the current wave of virus. In a pandemic situation, though the mutation rate of Corona virus is comparatively lower than Influenza virus, it infects billions around the world and chances are high for nature to experiment various mutations (some of them can escape from the current vaccines). Many vaccine manufacturers are already preparing booster doses that may protect from emerging variants.
Blood-clots and the vaccine link
In a record time science came up with several efficient vaccines and the whole world is engaged in the biggest vaccination program in the history of mankind. More than a hundred vaccine-associated blood clots were officially reported in EU and US after jabbing millions of doses of COVID-19 vaccines, and those vaccines were on pause and public demand for those dropped in many countries. Two scientific studies showed possible links between the Oxford vaccine with the rare blood clots. Further investigations on vaccine associated blood-clot patients detected antibodies against platelet factor-4 (PF4) in them, proposing a mechanism through antibodies against PF4, inducing an autoimmune response and clots. To prove the causal link between these rare phenomena and the viral vector or other vaccines further scientific investigations are warranted. European Medicines Agency (EMA) concluded that unusual blood clots with low blood platelets should be listed as very rare side effects of Oxford/AstraZeneca/Covishield (1 in 100,000 vaccinated people), a viral vector based COVID-19 vaccine.
Based on similar rare episodes in the USA, another viral vector vaccine Johnson & Johnson/Janssen was also on a temporary pause. Recently, following a thorough safety review, FDA and CDC recommended to lift the pause regarding the use of the J&J COVID-19 vaccine and use of the vaccine may resume. Both the EMA and FDA resonated in their decisions that the vaccine’s known and potential benefits outweigh its known and potential risks in individuals 18 years of age and older. EMA reminded the possibility of very rare cases of blood clots combined with low levels of blood platelets occurring within 2 weeks of vaccination. So far, most of the cases reported have occurred in women under 60 years of age within 2 weeks of vaccination.
In India, the mass vaccination program is now extending to younger ages from May onwards, and the health system would be vigilant and expect the occurrence of such rare events of blood-clots (if there is a causal link between vaccine and blood-clots) since Covishield is the major COVID-19 vaccine currently being rolled out. Such case reports may create panic and decelerate the vaccination program, hence public awareness on these rare side effects is vital. Though chances of this unusual blood-clot are rare, EMA recommends being aware of the symptoms within weeks after the injection, to seek medical attention. Patients should seek medical assistance immediately if they have the following symptoms in the weeks after the injection such as shortness of breath, chest pain, swelling in leg, persistent abdominal (belly) pain, neurological symptoms, including severe and persistent headaches or blurred vision, tiny blood spots under the skin beyond the site of injection. The pause, safety review and subsequent lift suggests that the surveillance system is functioning efficiently as they were designed (that too after identifying even rare cases).
How to get out of this mess?
Getting back to ‘pre-pandemic period’ will take time. With nearly half a dozen effective vaccines in our catalog, it would take lesser time than we first anticipated. Currently, two effective COVID-19 vaccines (including indigenous Covaxin) are spearheading the humungous vaccination program in India. An effective COVID-19 vaccine protects you from critical conditions and keeps you safe. Even if you are vaccinated, one can get mild or asymptomatic disease and can spread the bug. You must wear mask to protect the vulnerable from you, even if you are vaccinated, “masks are not theater”- as Fauci says. If you care, follow the mitigation measures like social distancing, masks, hand hygiene, avoiding indoor gatherings etc. until a significant population is vaccinated. Several vaccines against deadly diseases do give long-term immunity. This pandemic is only a year long, predicting what happens in 10 years’ time is not Science (Scientists are not fortunetellers with crystal ball!). Some variants may escape current vaccines (such variants may be out there already), and in that case we may need 3rd dose or dose every year as flu vaccine.
Yes, the fatality rate of the disease is low, the disease is mostly dangerous for vulnerable (though it may vary with some variants). But when it becomes a pandemic, it infects and kills in millions, suffocates the health system and eventually kills more vulnerable. With vaccines we can reduce the deaths significantly. Go for a COVID-19 vaccine that is offered by the health system. Herd immunity for infection may not be possible but herd immunity to prevent deaths is possible. Quoting Roberto Burioni here “the Earth is round, gasoline is flammable, and vaccines are safe and effective, all the rest are dangerous lies.”
References
https://outbreak.info/resources/2021.04.22.440932
https://www.gisaid.org/hcov19-variants//
https://www.ema.europa.eu/en/news/astrazenecas-covid-19-vaccine-benefits-risks-context
https://www.nejm.org/doi/full/10.1056/NEJMoa2104882
https://www.nejm.org/doi/full/10.1056/NEJMoa2104840?query=recirc_curatedRelated_article
