
Corona wave and its resurgence
In spite of the predictions that, this viral fever may subside in later months from its start, COVID-19 is surging worldwide even after 7 months. Earlier it was more prominent in the Northern hemisphere now it is escalating in the South. While Europe is starting to breath after the destructive first wave, several states in US, South America are still suffocating from the extended first wave. COVID-19 is flaring up in the second most populated country-India and hope the wave won’t transform into a tsunami. Now, Europe is cautiously back to business. Tourist places are filled mostly with locals this year, masks are not mandatory in many places, but social distancing is practiced to an extend in public transport and restaurants. When you take a closer look at the daily cases these days, you can see a resurgence in many of these countries. Only time will say whether this are the early signs of a ´second wave´? Until a vaccine arrives, with our knowledge gathered so far about this virus and disease, we must be able to test and contain those potential hotspots to avoid vast outbreaks and a nation-wide lockdown.
Vaccine is the way out!
Since our fishing experiments on repurposed drugs is not giving very promising results, our hope is on an ´efficient vaccine´. Nearly a couple of hundreds of vaccine candidates are on different levels of pre-clinical and clinical trials. The process of vaccine approval takes long time (to find its immunological response, the dose, moreover the efficiency in the real battlefield). Due to the urgency, supported by modern technology, we are seeing fast-track processing of several vaccine candidates. Hopefully we may start distributing vaccine/s against this disease before the end of this year (may have to wait several months, until everyone gets their priming dose). Preliminary results from different vaccine candidate came out recently and are promising. Many vaccine candidates are exhibiting proper immune responses, which is really exciting. Oxford/Astra Zeneca/Serum Institute of India, Sinovac, Sinopharm and Moderna are the lead runners in this Marathon and entered into the crucial efficiency test (Clinical phase 3) in the field with thousands of participants in many countries. Fingers crossed!
Airborne route of transmission
A group of international Scientists recently made commentary that urges the medical community, public-health authorities to acknowledge the potential for airborne transmission through aerosols (tiny droplets that can linger in the air for several minutes). WHO acknowledges that in crowded, poorly ventilated spaces, short-range aerosol transmission cannot be neglected, but waiting for more evidences on the infectivity of these aerosols? SARS CoV-2 virus spreads mainly through droplets on contaminated surfaces generated by coughing, sneezing and talking. Droplets travel short distances and drop quickly from air to the surfaces due to its density. The viruses from surface droplets are transferred by people’s hands. Hence the relevance of washing hands and using sanitizer to control the transmission. In crowded, poorly ventilated indoor spaces aerosols with viruses may form. Whether these aerosols carry ´viable viruses´ that can cause illness is something we are still waiting to prove. Clear recommendations from health authorities for physical distancing, wearing masks, avoiding indoor gatherings may control aerosol transmission if it is proven.
Herd immunity by natural infection is attainable, but slow
A serological study from Spain on COVID-19 patients got much attention. Their data (only 5% of the population got infected) was misinterpreted to a large extend and social/media spread the wrong message that herd immunity is ´not attainable´ for COVID-19. The study looked at one arm of immune response to detect the prior infection (antibody against SARS CoV-2) while did not test the T-cell mediated immunity, which plays a vital role in fighting against this virus. Sweden, who took a different approach than its Nordic neighbors could not achieve immunity in large percentage of population (mere 6% of population developed antibodies to COVID-19). Nearly 10% of population in Stockholm (worst affected area in the country) had developed antibodies to COVID-19. Similarly, the worst hit New York city could infect nearly 20% during the disastrous first wave. The data shows with strong mitigation steps that countries adapted, we could contain the virus and resulted in lower percentage of infected cases during the first wave. Note, most of the studies are analyzing only the antibodies in the COVID-19 survivors, while recent studies suggest that crucial role of cell mediated immunity (another path that our body´s immune system uses to combat pathogens). These data can be correctly interpreted as that herd immunity (target estimated as over 70%) is achievable but slowly, only through multiple rounds of natural infections through the population, at the cost of more millions of lives.
HCQ, how many more nails we need in that coffin
An anti-malarial drug hydroxychloroquine/chloroquine (HCQ), effective in some chronic disease conditions also (like arthritis, lupus) became very controversial during this pandemic. Some ´preliminary observational data´ on its effect to treat COVID-19 was reported from China followed by another one from France (later retracted) and was quickly blown out of proportion as the ´magic bullet´ and US President became the brand ambassador for this ´gift from Heaven´. FDA issued a quick emergency use authorization based on the ´evidences´ at that time. Due to overhyped anecdotal evidences as ´the anti-COVID-19 drug´, people all over the world started stockpiling this drug, posing a huge problem for those patients relying on this drug for their chronic clinical conditions. Scientific community was cautious and suggested for the scientific evidences from clinical trials. It is hypothesized that HCQ blocks a pathway that helps this virus to enter and release its content into the infected cell.
Several studies came out during this pandemic and now we can have a conclusion on this so called ´anti-Corona drug´. Verdict from many clinical trials was against the claims from this magical drug. A study from Spain did not find any significant benefit from HCQ on illness, Recovery trial in UK pointed out no clinical benefit on hospitalized COVID-19 patients, a combined study from the USA/Canada also showed that HCQ did not prevent illness in virus exposed individuals. Recently two articles in journal Nature, reported failures of HCQ as anti-viral drug, when investigated using lung cells in a culture-plates and in non-human primates. Though a plethora of evidences against using HCQ against COVID-19 are already present, many anecdotal and observational evidences are still coming. Based on interim trial results on HCQ and lopinavir/ritonavir that showed little or no reduction in the mortality of hospitalised COVID-19 patients compared to standard of care, WHO decided to discontinue the trials with immediate effect. Dr. Anthony Fauci recently said ´valid’ scientific data shows HCQ is not effective in treating coronavirus. Even with surplus of valid scientific evidences against HCQ, if one still claims a marginal benefit from HCQ administration based on anecdotal evidences, the risks associated with its administration could negate any such benefits (if at all!) in COVID-19 scenario.
Remdesivir, another potential repurposed drug is not giving exciting results. A clinical study from China on this wonder drug suggested no significant clinical benefits. Another study showed that this drug shortened the duration of illness. Currently, the results do not suggest it as ´the cure´ for COVID-19.
Relapse, is that possible?
One disturbing question that comes quite often is whether there is relapse of COVID-19? Whether one can get the COVID-19 illness twice? Earlier there were reports of reinfection of the SARS CoV-2, weeks after the first infection. These could be rare incidents on immunosuppressed individuals or false detection by tests. Note, some viral infections/vaccines give immunity for life long, some for years while some for weeks. So still we are on the learning curve about this virus’s ability to invade the system multiple times. A decline in levels of antibody weeks after an infection is quite normal that does not mean we are prone to same illness again, note that we have other defense mechanism to protect us like cell-mediated immunity. Which means that this arm of protective immunity may last longer and can prevent or ease the symptoms on a second infection (if it happens).
Cell-mediated immunity: our body will not forget SARS-CoV-2 infection
Antibodies are specific warrior proteins produced by our defense system (triggered by the presence of a pathogen or its proteins or a vaccine) to selectively destroy the invading pathogens. Our immune system is very efficient also in directing specific cells (like activated T-cells) to scavenge the pathogens or even kill the infected body cell. Once the virus enters our system (a cell), the resident guard cells recognizes the signals of the infection (viral proteins or chemical signal calls from an infected cell). The activated guard cells will initiate an immune response producing antibodies and cells to neutralize/destroy the invading pathogen. Within days after a viral infection our body will create tailored antibodies and immune cells, which eventually inactivate the pathogen and eventually these immune responses subside. But the memories of this attack retain in specialized memory immune cells. Even after several years, upon a second attack by the same pathogen, these memory immune cells get quickly activated, produce antibodies quickly and protect our body. We have a strong immune system, and have a repertoire of memory immune cells, a reason why we are rescued from several pathogens that we encounter daily.
Recently some scientific studies came out which suggest the cell-mediated response will have a major role in our combat against SARS CoV-2. Most studies analyze the antibody profiling due to the availability of tests. Routine clinical analyses of cell-mediated immune response are not practical. On several weeks post-infection, the antibody level against that pathogen goes down, while memory immune cells remain. On testing serum antibody level on a COVID-19 survivor at a later stage may show less (depending on the sensitivity of the test) antibody titer. Current studies point to the necessity to understand the cell-mediated responses to SARS-CoV-2 infection, as well as in understanding the immune response of COVID-19 candidate vaccine clinical trials.
Experience matters! Pre-existing immunity to SARS CoV-2
Interestingly, now we have convincing evidences (from various scientific groups from different countries) that, a significant percentage of SARS CoV-2 unexposed population (20-50%) has T-cell immune response to SARS CoV-2! These analyses were done on blood samples (collected from 2015-2018, long before COVID-19). The speculation is, this could be a cross-reactivity to circulating ‘common cold’ coronaviruses in those un-exposed. Or whether it indicates this virus was circulating much earlier than we thought? This surprising, but significant pre-existing T cell immune response to SARS-CoV-2 may elicit quicker immune response to these immune privileged population when they encounter SARS-CoV-2. The observations are compelling us to hypothesize that this could be a reason for less severe cases in a large percentage of general population (due to preexisting immunity donated by previous coronavirus infection episode/s). Also, these reports caution us to screen whether the participants in various vaccine trials are already having the advantage of this preexisting immune response to this virus. Further studies are warranted to identify the source pathogen for this unprecedented T-cell response to SARS CoV-2 and clinical relevance of this important observation.
A solution for the spreading problem- daily testing to find the ´infectious´
As the primary wave is shifting towards the Southern hemisphere, and there is possibility of a subsequent wave in recovered countries (herd immunity is no way near) we should be prepared for worst case scenario in coming winter. It is impossible to live in a bubble with borders closed until we are ready with vaccine. Extending nationwide lock down for more months is not always the ideal solution, since repercussions are already visible even in developed world. Developing world don’t have the luxury to have longer lockdowns. Economic burden, mental health issues, absence of social life are some of the backlashes of stricter steps like lockdowns. Daily testing to find out the ´infectious´ and isolating them is the method to control spreading. ´Behavioral/social vaccine´ such as, using masks, keeping social distancing, avoiding gatherings, practicing hygiene measures and closing down hotspots (if necessary) are the proper ways to fight until we have the COVID-19 vaccine in our hands. Country wide lockdown is drastic and is not a feasible idea in a long run.
Expensive-limited test is not a solution, but a cheap-rapid daily test is!
Test, Trace and Isolate (TETRIS) is the ideal strategy to fight this hidden enemy. Though it is only 7 months, we learned much about this disease and its causative agent. Recent studies point out that this disease spreads significantly through pre-symptomatic and asymptomatic patients. Moreover, the viral load peaks up and infected person transmits his virus through droplets to others even before any noticeable symptoms (up to 2-3 days before any symptoms!). Hence by the time one realizes by symptoms that he may be infected; he might have done the damage by spreading his virus to others. This is one of the main reasons why it is difficult to control spread of this ´successful´ virus (a virus from Wuhan could multiply in astronomical order and infect 18 million worldwide within a span of 7 months!). So, catching the infected who can transmit the virus (infectious), tracing their contacts and isolating them (TETRIS) is the best strategy to control the spread.
If there is a way to warn an infected person at an early ´infectious´ or ´transmitting´ stage, we can reduce the extend of spread. Currently there is long queue for the tests and long waiting time for the results (from days to weeks depending on the country), which is not effective at all if we consider the nature of this infection. We are obsessed with the sensitivity of the test and qPCR becomes the expensive gold standard (qPCR is very sensitive in detecting minute amounts of viral RNA fragments in a sample). The machine to run the test and reagents are expensive, and it requires expertise to conduct and interpret the results. Remnants of the viral RNA, at early stage of the infection or at the later phase when infection subsides, could be detected by the sensitive qPCR. In either scenario above, detecting few copies of viral RNA does not mean that the person is spreading the disease.
I will try to explain it in a bit more detail (in an oversimplified manner, for the general audience) about the issues with the current COVID-19 tests. Currently we use RT-PCR reaction and use the expensive qPCR machine to amplify and detect the viral genetic material in a swab sample (if interested, you can read the earlier blog for more details https://viralvector.design.blog/2020/03/25/war-against-a-virus/ ). Suppose by qPCR (the highly sensitive test currently we use) we can detect as low as 100 viral particles from a swab (note: qPCR detects RNA fragments, hence sometimes remnants of inactive viral particles are also detected). Detecting such a low number of viral particles in a sample using this sensitive method is fantastic, but the question is whether it is necessary? Let’s assume a threshold viral load (e.g. 10,000 viruses) is needed for a person to successfully spread the virus through the droplets to next person. A lower viral particle number from the test means the person may be initial phase of infection or had surpassed the peak infection (now at the later phase of illness) but he is not a risk for transmitting this viral disease. For those who care the details, the Ct value in qPCR is what matters here; it gives a relative measure of the viral RNA in the sample. Hence it may be irrelevant to detect the minute number of viral particles in an infected. On the other hand, it is more relevant to determine whether the person is in the range or above the threshold viral load, for transmitting the disease. For that purpose, a less sensitive test is more than enough, a test that can faithfully detect nearly 10,000 viruses (number just as an example) or above will serve the purpose.
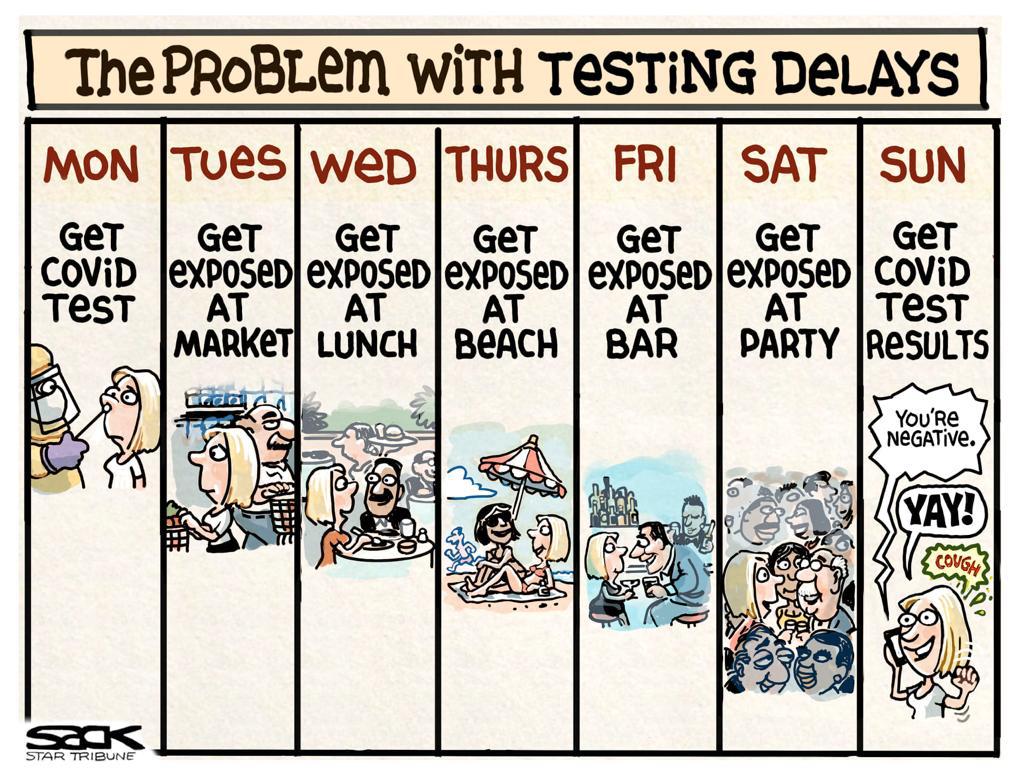
The question here is do we need such a sensitive but tedious, expensive and less frequent testing solution to control this disease? Prof. Michael Mina at Harvard T. H. Chan School of Public Health has a cool strategy for this problem. He suggests a less expensive, less sensitive test but more frequent testing (daily test) as a solution to prevent viral spread in an efficient manner than expensive, time consuming, less frequent test that currently we are deploying to fight against this disease. A person who is giving swab for test on Monday may know his result only after several days, in between the wait he may get exposed to a virus infected person (see the cartoon below). Conversely, if the person is in infectious phase while giving swab for test, due to delays he may be distributing his virus to several. To avoid such scenarios through which extensive transmissions are happening, a cheap-daily testing becomes necessary.
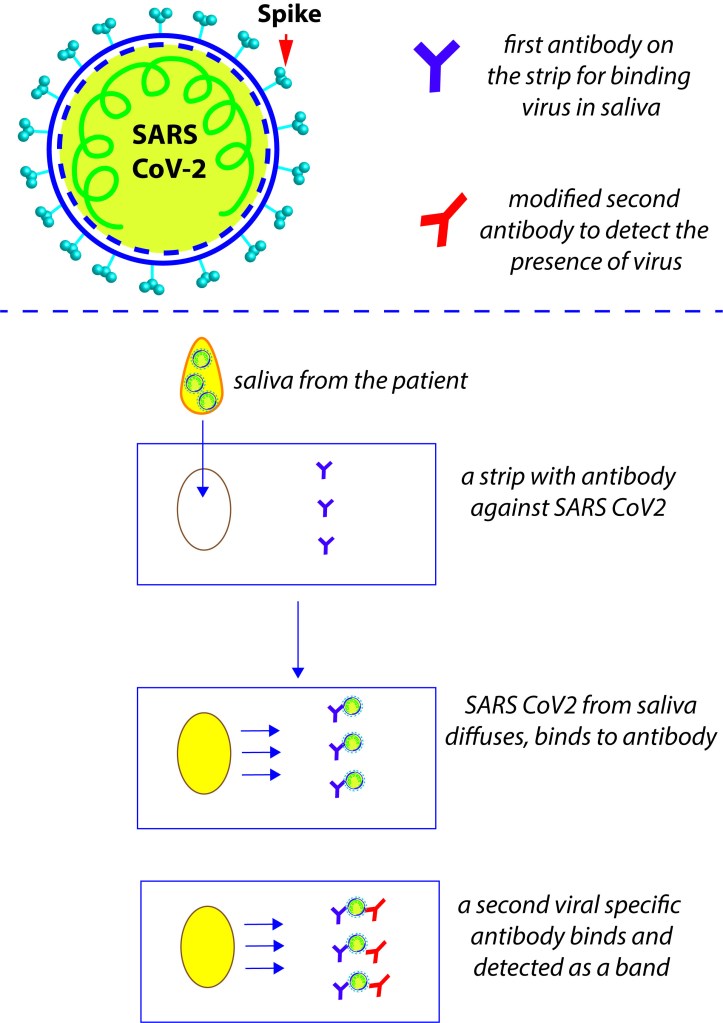
A lateral flow assay strip (similar to pregnancy detection strip) that detects viral antigens from one’s spit may be the one warranted. Here is the oversimplified version of the rapid antigen test for daily use (see the diagram below). Such paper strips use antibody against the SARS CoV-2 printed on paper strips to detect the presence of viruses in the sample. The subsequent reaction chemistry with another modified SARS CoV-2 antibody will exhibit the presence of virus as clear colored bands. One does not need any expertise in conducting this test or interpreting the results. Spit on the strip (no unpleasant nasal swabs or painful needles), add some solutions, wait a few minutes, if there are band/s- you are tested positive, isolate! If there are no bands- you are tested negative, and free to cautiously get back to work, but remember to test tomorrow. Moreover, such a test will help one to decide whether he needs to go out for his daily life activities or self-isolate himself and be a responsible person by not spreading the disease to vulnerable. TWiV lead by Prof. Vincent Racaniello and team, (https://www.microbe.tv/twiv/) supports this 1-dollar daily-rapid antigen test as an effective solution for this fight. Such a daily cheap test (compared to qPCR) will have huge impact on the current testing strategies in 3rd world and preparing all of us in case of probable subsequent waves. This test will help to get the workforce back to their jobs, kids back to their schools and ultimately save the vulnerable from getting exposed to the infected.
LAMP based testing
This is also an alternative testing approach called LAMP (Loop mediated isothermal AMPlification). Abbot ID Now machine that Mr. Trump endorsed, uses a similar isothermal reaction mechanism. The LAMP PCR reaction chemistry is complicated but quicker and cheaper than qPCR. But it is not as cheap as a 1-dollar antigen detecting strip assay that Prof. Michael Mina was proposing. As the logic above mentioned, such a test is more than enough to screen those infectious who are with viral load above the threshold to transmit the disease.
Children can transmit disease!
In many countries the schools reopening after the summer holidays. The million-dollar question is whether the kids can transmit COVID-19? Now there is overwhelming evidence that kids or youngsters don’t get seriously ill compared to adults. That does not mean this virus is not getting transmitted through them. A recent study from South Korea showed the school aged children aged 10-19 years can spread the disease at a rate similar to adults. COVID-19 transmission rate was 18.6% for household contacts of school-aged children (10-19 years) and 5.3% for household contacts of children 0–9 years. Note that they analyzed these transmissions in the middle of mitigation. Their data shows clearly that, kids also can transmit the disease and sufficient precautionary measures should be taken while reopening the schools. Another recent study conducted in the USA on a small cohort of patients shows that SARS CoV-2 viral RNA levels in infected children are similar to adults, reinforcing the common notion that children drive spread of respiratory and gastrointestinal illness in the population, and COVID-19 transmission may not be different.
Comparing Sweden´s approach to other countries
Extrapolating the controversial approach carried out by Sweden to other settings may be foolishness. Sweden has several advantages to begin with when they tried this bold strategy; such as low population, high standard of living, healthy population, efficient public health system, most households with one generation etc. Even with such favoring conditions, Sweden suffered a lot with their out-of-the box experiment. Nearly 5700 precious lives got sacrificed during the first wave of this hidden enemy, attaining a mere 6% percentage infected (10% showed serum antibodies in Stockholm- worst affected area in the country) had developed antibodies to COVID-19 and economical backlash as rest. Note, here analyses were on the antibodies against COVID-19 and not on the cell-mediated immunity arm (hence percentage will be more than reported, but no way near to attain the herd immunity). 570 deaths/million in Sweden, is similar to nearly 780,000 deaths in a country like India (would be even more if you consider the huge population density and other conditions that makes it a favorable playground for this bug). For a better ´apples to apples´ comparison, let’s take a look at the number of Scandinavian neighbors Denmark (106 deaths/million) and Norway (47 deaths/million), who took stricter lock down approach at the initial phase.
Better be prepared
First round of COVID-19 provided infection to only less than 5-10% of the population even in many worst affected countries. Unfortunately, this means herd immunity through natural infection is far away and may need to multiple waves of infection to attain it (if that is the way, this virus will take lives of more millions). Until an effective vaccine arrives (due to the absence of an effective drug treatment), we have to strictly follow behavioural and social mitigation measures to protect the vulnerable. Mitigation until an effective vaccine arrives may be the only possible way out. First wave of infection exposed our weakness in pandemic preparations. Learn from the mistakes, prepare the testing and hospital facilities, stockpile gloves, masks, PPEs for health workers, essential medicines, ventilators etc. In order to prevent viral spreading, we need to detect, isolate and trace contacts of the infected at the earliest. We need to catch those who are infectious at the right time. Limited, less frequent and expensive current strategy of testing is targeting the ´detection´ of virus and not focusing on ´infectivity´ of the patients, hence not appropriate to harness this viral transmission. A cheap, rapid and daily testing method on the other hand is more efficient for controlling viral spread. Now, with the schools reopening, people getting back to work after holidays and to their normal life, things are going to be easy for this virus to have a second round of carnage. Those countries survived the first wave with less injuries should not be under the false impression that ´we are done with this virus´, understand that this virus is not done with us yet, better be prepared!
References
Updates on COVID-19
https://science.sciencemag.org/content/369/6503/510
Airborne transmission
https://academic.oup.com/cid/article/doi/10.1093/cid/ciaa939/5867798
HCQ results, do we need more evidences?
https://www.nature.com/articles/s41586-020-2575-3
https://www.nature.com/articles/s41586-020-2558-4
https://www.nejm.org/doi/full/10.1056/NEJMoa2016638
Remdesivir results
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)31022-9/fulltext
https://www.nejm.org/doi/full/10.1056/NEJMoa2007764?query=featured_home
LAMP testing
Children can transmit COVID-19
https://wwwnc.cdc.gov/eid/article/26/10/20-1315_article
https://jamanetwork.com/journals/jamapediatrics/fullarticle/2768952
Relapse of COVID-19 is that possible?
https://www.bbc.com/news/health-52446965
TETRIS
https://asm.org/Podcasts/TWiV/Episodes/COVID-Tetris-Test-trace-isolate-TWiV-614
Frequent daily testing (Prof. Michael Mina)
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7314112/
https://www.medrxiv.org/content/10.1101/2020.05.01.20086801v1
https://www.medrxiv.org/content/10.1101/2020.06.22.20136309v2
T-cell mediated immunity and neutralizing antibody
https://www.nature.com/articles/s41586-020-2550-z
Pre-existing immunity
https://www.nature.com/articles/s41577-020-0389-z
Vaccine preliminary results
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)31604-4/fulltext
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)31208-3/fulltext
https://www.nature.com/articles/d41586-020-02154-2
https://www.nature.com/articles/d41586-020-02174-y
Herd immunity is attainable but slow!
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)31483-5/fulltext
https://www.medrxiv.org/content/10.1101/2020.06.28.20142190v1
Timing of shedding and transmission of SARS CoV-2

I like the optimism that a vaccine might be ready by the end of this year 👍
But the next question is, what’s going to be the accessibility of that for developing countries. Hoping that India can be helpful with that.
LikeLike
Thanks 🙂 Even if the vaccine/s get ready, agree that it may be difficult that all get a shot soon (there may be some way of cherry picking). Some vaccines need boosting even, so multiple shots. Anyway, vaccine manufacturers are gambling, by already making enough doses so that they can have a quick start as soon as the vaccine is approved.
LikeLike